


11 Signs It’s Time to Get Your Moles Checked Out by Your Dermatologist,
Do you have moles? They are extremely common, so having them is not unusual. Although most moles are harmless, some may become cancerous. For this reason, it’s crucial to keep

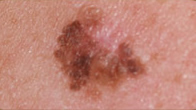
3 Warning Signs of Melanoma Dermatologists Wish You Knew and Didn’t Ignore
Skin cancer is the most common cancer in the U.S. One in every five Americans will get skin cancer in their lifetime. While melanoma is the least common type of